Written by:
Penelope Rafouli-Stergiou, MD, PhD
Director of the Cardiology Department, Therapis General Hospital

The latest guidelines for the diagnosis and treatment of patients presenting with acute coronary syndromes were presented at the recent European Cardiology Congress.
Cardiovascular disease (CVD) remains the most common cause of mortality and morbidity worldwide.
In the 57 member countries of the European Society of Cardiology (ESC) alone, there were almost 4 million deaths, while approximately 5.8 million new cases of ischemic heart disease were estimated in the last recorded year.
Acute coronary syndromes (ACS) are often the first clinical manifestation of CAD. They encompass a spectrum of conditions involving patients who present with recent changes in clinical symptoms or signs, with or without changes in the 12-lead electrocardiogram (ECG) and with or without acute increases in cardiac troponin (cTn)
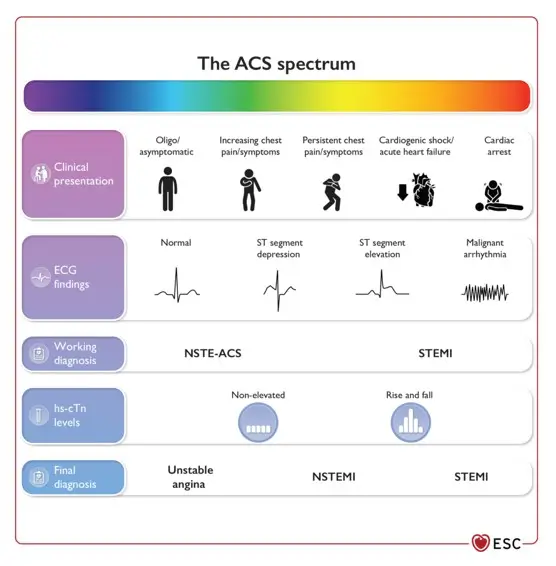
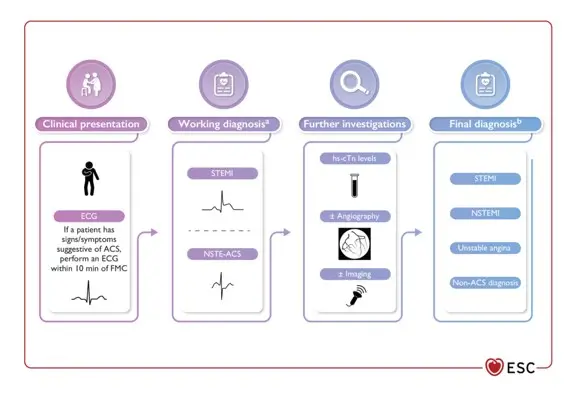
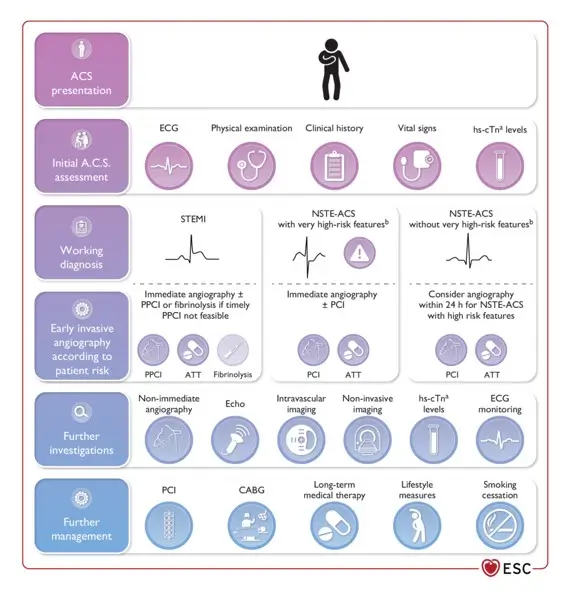
ACS is associated with a wide range of clinical manifestations, from patients with no symptoms at presentation to patients with ongoing chest discomfort/symptoms and patients with cardiac arrest, electrical/haemodynamic instability, or cardiogenic shock. Patients with suspected ACS are typically classified based on ECG at initial assessment. After that, patients can be further classified based on whether or not cardiac troponin is elevated, as shown in Figures 2 and 3. These characteristics (ECG changes and cardiac troponin elevation) are important in the initial triage and diagnosis of patients with ACS, helping to stratify and guide the initial treatment strategy
However, after the acute treatment and stabilization phase, most aspects of the subsequent management strategy are common to all patients with ACS. Although closely related, it is important to recognize that ACS is not the same as myocardial infarction (MI). Acute myocardial infarction is defined as necrosis of myocardial cells in the clinical context of acute myocardial ischemia.
Myocardial injury is another distinct entity, used to describe troponin release due to mechanisms other than myocardial ischemia and does not meet the criteria for AMI. Some causes of myocardial injury include myocarditis, sepsis, takotsubo cardiomyopathy, valvular heart disease, cardiac arrhythmias, and heart failure.
It is worth noting that acute chest discomfort — which can be described as pain, pressure, tightness, heaviness, or burning—is the main symptom raising suspicion of ACS and triggering tests included in specific diagnostic algorithms. Based on the description of chest pain, the symptom should be classified as cardiac, possibly cardiac, or possibly non-cardiac. The term “atypical,” which has been used until now, should be avoided. Equivalent symptoms include shortness of breath, pain in the epigastrium, left or right upper extremity, throat, or lower jaw.
Incorrect or delayed diagnosis is sometimes due to incomplete medical history or absence of symptoms. Symptoms such as prolonged chest pain (>15 minutes) and/or recurrent episodes of pain within 1 hour should prompt patients to seek emergency medical attention. Electrocardiographic monitoring should be initiated as soon as possible in all patients with suspected ACS.